As featured in Waterline Spring 2025
One Language, Two Professions: How we use the words risk assessment to mean very different things
By Elaine Cloutman-Green, Deputy Director of Infection Prevention and Control at Great Ormand Street Hospital
The world of healthcare is becoming both increasingly complex, and in response, increasingly requiring interdisciplinary approaches, as combined skill sets are needed to identify solutions. Nowhere is this truer than in the world of the built environment, where it is no longer possible to work in silo’s and deliver the best possible patient care and patient outcomes. Working within this shared space however is new to pretty much everyone, and there are frequently assumptions made about both baseline knowledge between fields and meaning when we are communicating amongst each other. Having worked within Infection Prevention and Control for over two decades, and having focussed on the built environment for at least 15 years, I thought it might be helpful to discuss where I’ve recognised that these assumptions have led to challenges, and potential patient impacts, during my practice.
Different meaning
Let’s start with the baseline, no one aims to provide risky or less good care. No one, no matter what their professional background, chooses to work in a hospital if they are not aspiring for the best outcome for patients. This is true whether you are nursing a patient one to one, or providing the essential care to the building in which they are housed. A one team approach has never been more important.
In my experience the problems tend to arise in the communication behind our practice. A non engineering example of this is when I discuss the fact that I am about to go off and undertake a HPV review. Many of my clinical colleagues would assume that I am leaving to speak about Human Papilloma Virus, whereas in fact I am probably going to talk to facilities about the use of Hydrogen Peroxide Vapour for cleaning within our rooms. The two things are very different, and yet, without being aware of the impact of our communication choices, it is easy to believe we have communicated our meaning when in fact we’ve just set very different expectations as to the event.
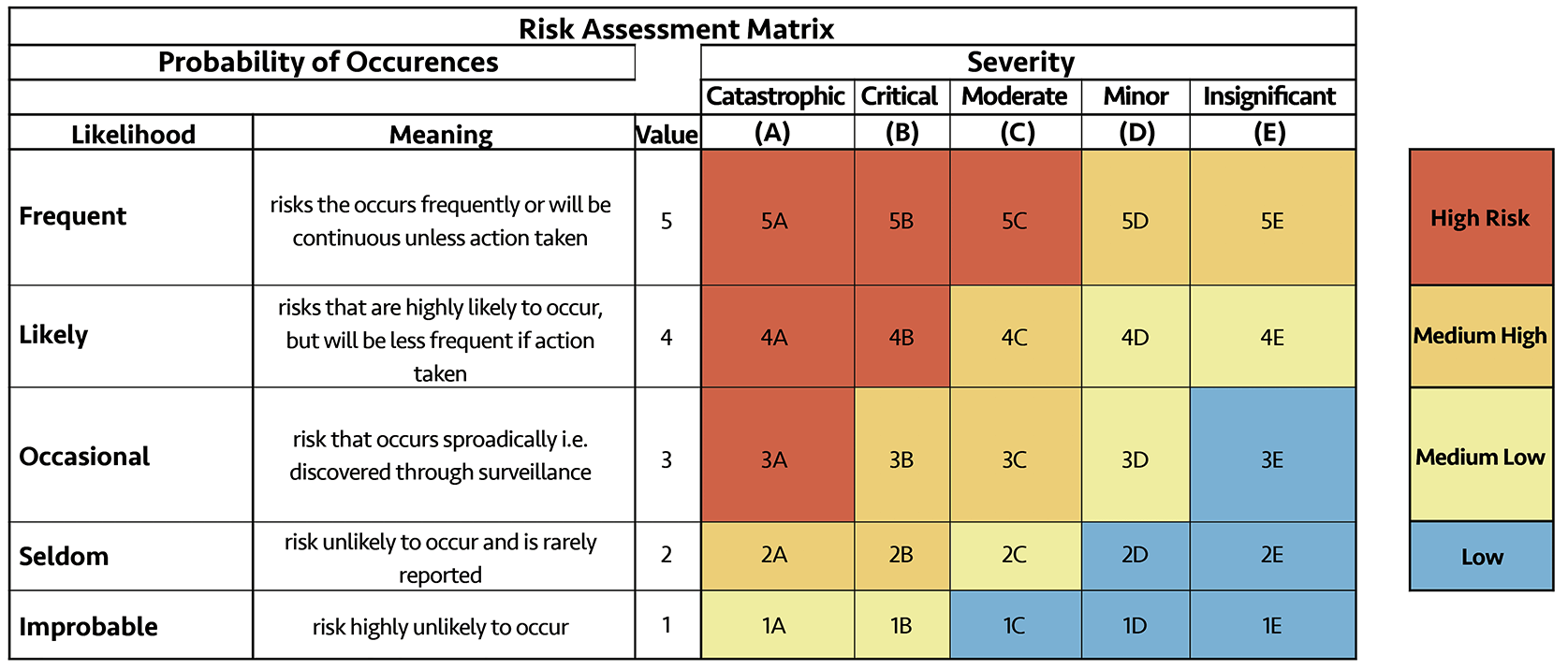
All of which brings me onto the use of the term risk assessment in healthcare. Traditionally when we talk about risk assessment, the thing that springs to the minds of most people is a 2 x 2 grid that lists both the likelihood of an event occurring and the severity of that event if it did happen. This kind of matrix is often presented to me when I request a risk assessment is undertaken by my estates colleagues linked to a particular event, or ongoing risk, alongside a set of mitigations.
The problem with this kind of response is that it often fails to capture the sort of response and detail that I am actually asking for when I request a risk assessment within a clinical context. The 2 x 2 approach aims to summarise a lot of different components into a simple score. Why does that matter? Well, without sufficient details I cannot then make decisions linked to what clinical mitigations or actions may be required to address the risk from a clinical perspective, thus enabling a holistic response.
Within a clinical context, when I request a risk assessment, I am normally looking for a much more narrative approach that will capture a wide variety of different components, all of which come together to support me in making decisions about how to manage, not just the individual patient, but the wider risk to patients, visitors and staff.
This use of the same language but with very different expectations, in terms of levels of and presentation of detail, can result in a misalignment which impacts how successful we communicate across disciplines and how successful we are at collaborating.
Different purposes
I also acknowledge that there are other forms of risk assessment undertaken by my Estates colleagues or external support, with items such as Legionella Risk Assessments being a key example. In this case I recognise that a substantial amount of information is collected. The format, and declaration as I am not an engineer, I am therefore far from being an expert, is usually in the form of a series of questions where compliance is scored against presence or absence. This form of risk assessment, where measurement is undertaken against a known standard in order to determine levels of uncontrolled variability or to identify gaps in certainty, we would normally refer to as an audit within the clinical setting. Which is another reason why confusion sometimes arises.
So why are clinical risk assessments different? What are they trying to achieve? I believe some of the reasons for the difference is because of the reasons the information is being sourced. As described, sometimes engineering risk assessments are linked to assessment against known standards or known risk. Frequently the opposite is true in a clinical context. The process of risk assessment is usually undertaken clinically as part of a deliberate attempt to collect more information, as more data means improved decision making, especially in scenarios that are complex or uncertain. This means that risk assessment in a clinical setting is undertaken to achieve very different goals, frequently when there is no standard, or to support complex decision making. This is described by O’Riordan et al (2011) in the Stacey Matrix, where appropriate management actions in complex scenarios are based on both the degree of certainty and level of agreement. The process of gathering data within clinical risk assessment aims to capture uncertainty and engage stakeholders to discern consensus.
Shared objectives
All of this brings into focus the question of how do we better align? Well, obviously the first step is to have conversations about what it is that we actually trying to achieve in order to gain clarity and develop shared purpose, rather than feeling like we are using terminology as a short cut. Understanding that we use the same language for different processes as we are aiming for different objectives, is a key step forward in this.
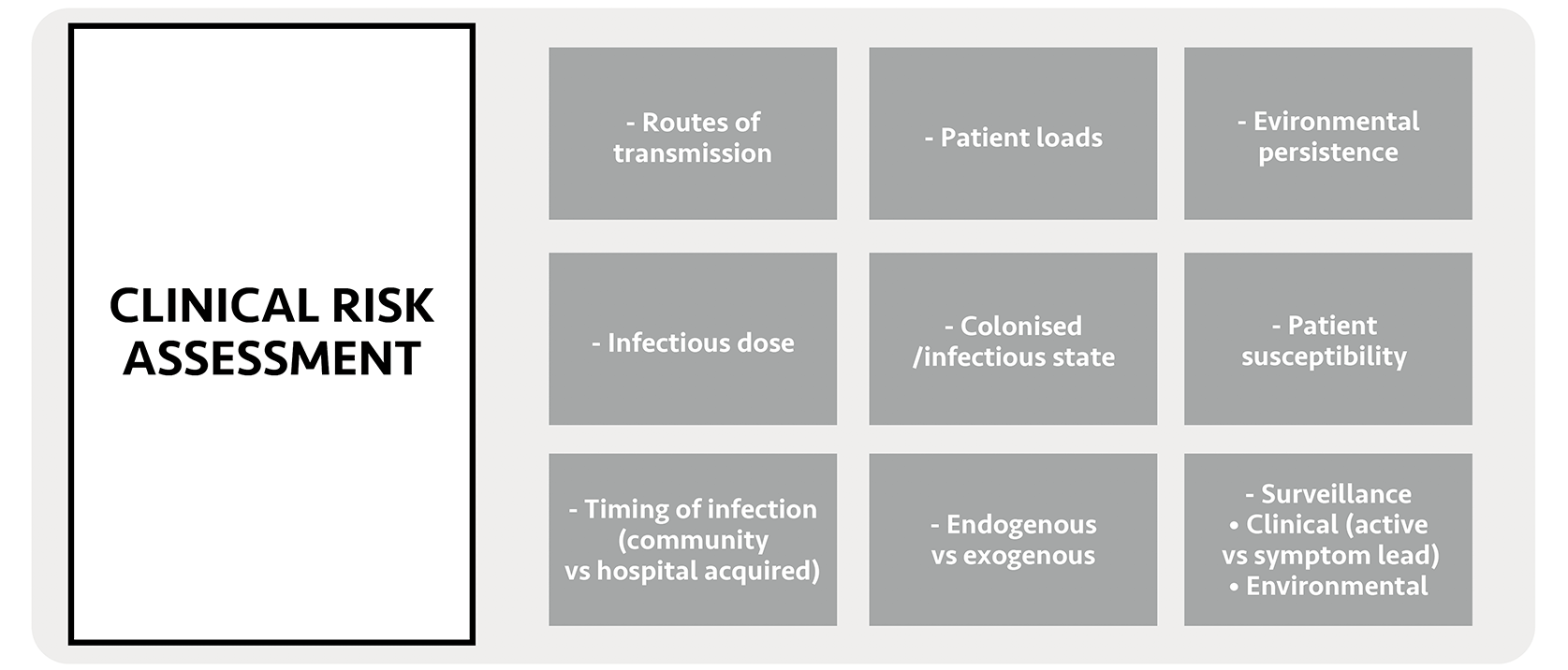
The other thing, I believe, is to acknowledge that maybe neither side has it entirely correct. In the clinical risk assessment image I show some key aspects of clinical risk assessment, but if you review it, you will see that it is missing some key components, such as the built environment. The same can be said for both of the commonly utilised engineering risk assessments, which may be too focussed on organism and built environment, without truly bringing in the human factors side of discussion. What I believe is that we need to be working towards a new triumvirate, where aspects of built environment, organism involvement and patient/human considerations are all included.
Healthcare environments are complex, organisms are constantly changing, and human beings bring a level of unpredictability into any decision making. Not only that, but these environments are also dynamic and change, not just by the day or season, but sometimes by the hour as staff shifts change and patient populations alter. In my world, a four year old is not going to use their space in the same way as an 18 year old, and a Klebsiella will behave very differently to a Legionella. We are not going to alter the complexity of these scenarios by ignoring the fact that they are there, so the best way forward is to embrace it. As for risk assessment, let’s start by saying what we mean and begin those discussions better by finding each other in our different professional silo’s. Let’s dig deeper to check that the words we are using are from the same language and acknowledge that, occasionally, we act as tourists in each other’s strange and wonderful lands.